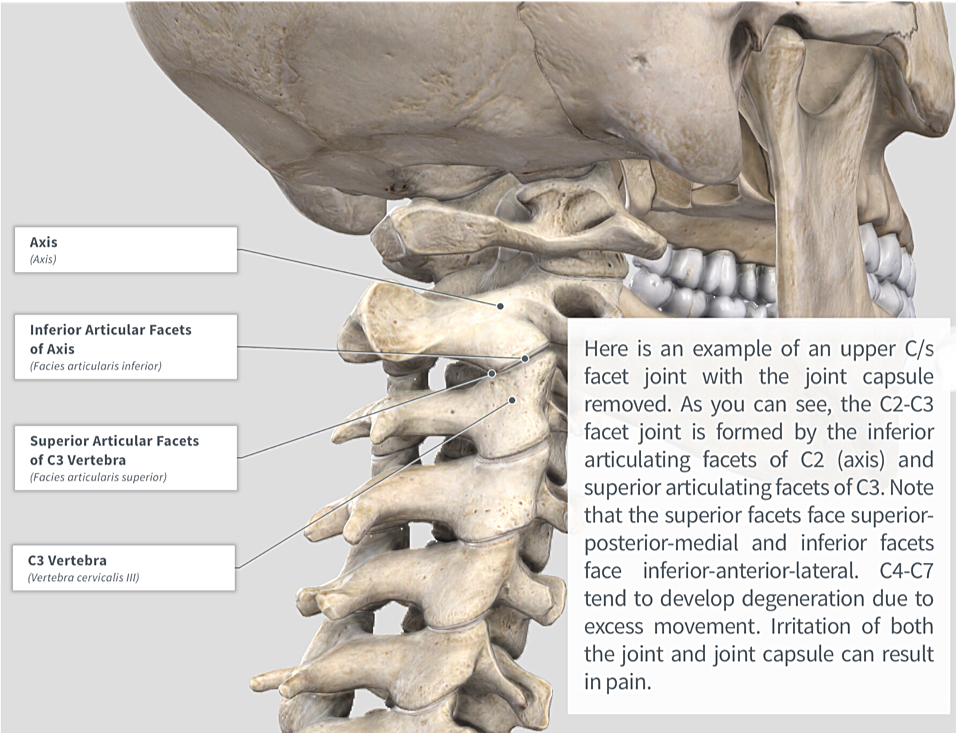
From anatomy to discovering the patient!

22% to 70% of the population will have neck pain some time in their lives
At any given time 10% to 20% of the population reports neck problems, with 54% of individuals having experienced neck pain within the last 6 months
Prevalence of neck pain increases with age
Most common in women around the fifth decade of life
See more prevalence information in the Clinical Pattern Recognition: Orthopaedics app here
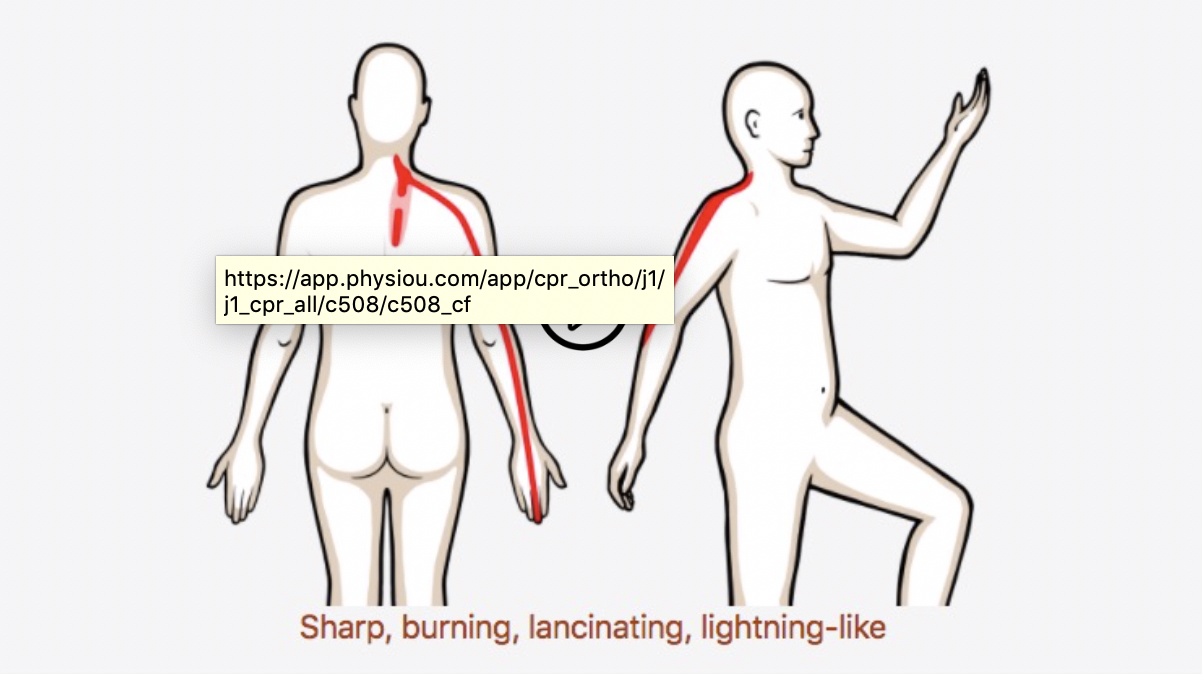
Meet the 5 common neck pain patients from the Clinical Practice Guidelines!
Clinical Pattern Recognition
Click on the pain pattern to learn about the patients and develop your clinical patterns!